
Exploratory analysis: Quality of life data
FKSI-19 patient-reported quality of life
Mean score numerically maintained near baseline with CABOMETYX® (cabozantinib) + OPDIVO® (nivolumab) for over 1.5 years1
Total score
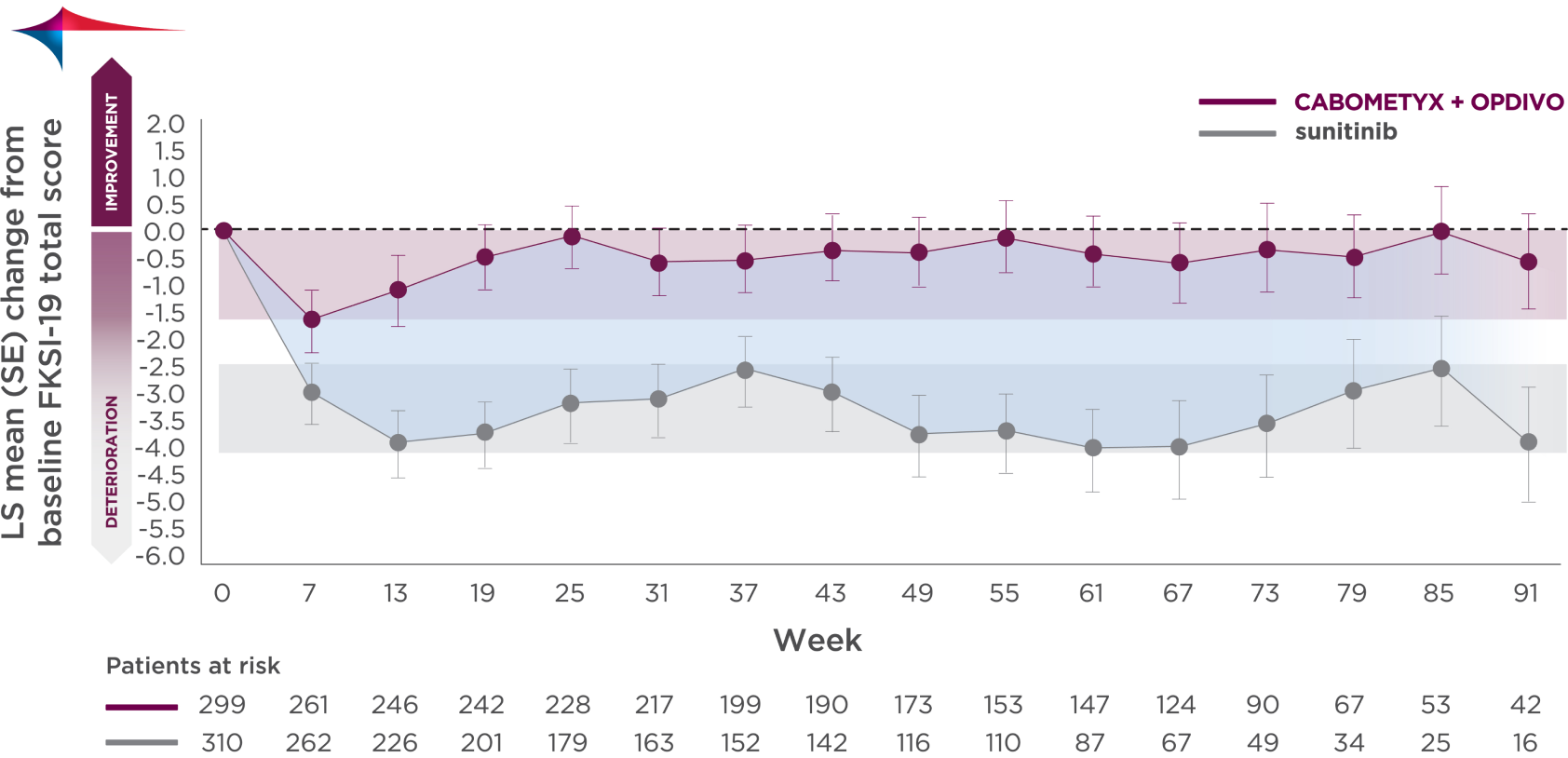
The clinical significance is unknown.2
Patients responded to statements on 7 domains3,4
- Pain
- Fatigue
- Pulmonary symptoms
- Bowel/bladder symptoms
- Nutritional health
- Psychosocial functioning
- Treatment side effects
- Baseline mean FKSI-19 total scores were similar between groups2
- >90% questionnaire completion rate at baseline in both groups; ≥80% completion rate at all time points through at least Week 91 in both groups2
Mean changes from baseline for the FKSI-19 and subscales were prespecified. Least squares mean used above was done post hoc.2
The FKSI-19 total score scale and 3 subscales (disease-related symptoms, treatment side effects, and functional well-being) were collected to measure tumor-specific HRQoL. Change from baseline was assessed with the use of descriptive statistics, based on a linear-regression model for repeated measures that controlled for treatment group, time point, baseline patient-reported outcomes score, and the stratification factors (IMDC prognostic risk score, tumor PD-L1 expression, and geographic region). "Patients at risk" denotes ITT patients with baseline plus at least 1 post-baseline HRQoL assessment with nonmissing, patient-reported outcome data. Time 0 indicates baseline.1,2
FKSI-19 disease-related symptom (DRS) subscale
Mean score numerically improved above baseline after Week 7 with CABOMETYX + OPDIVO for over 1.5 years1
DRS subscale
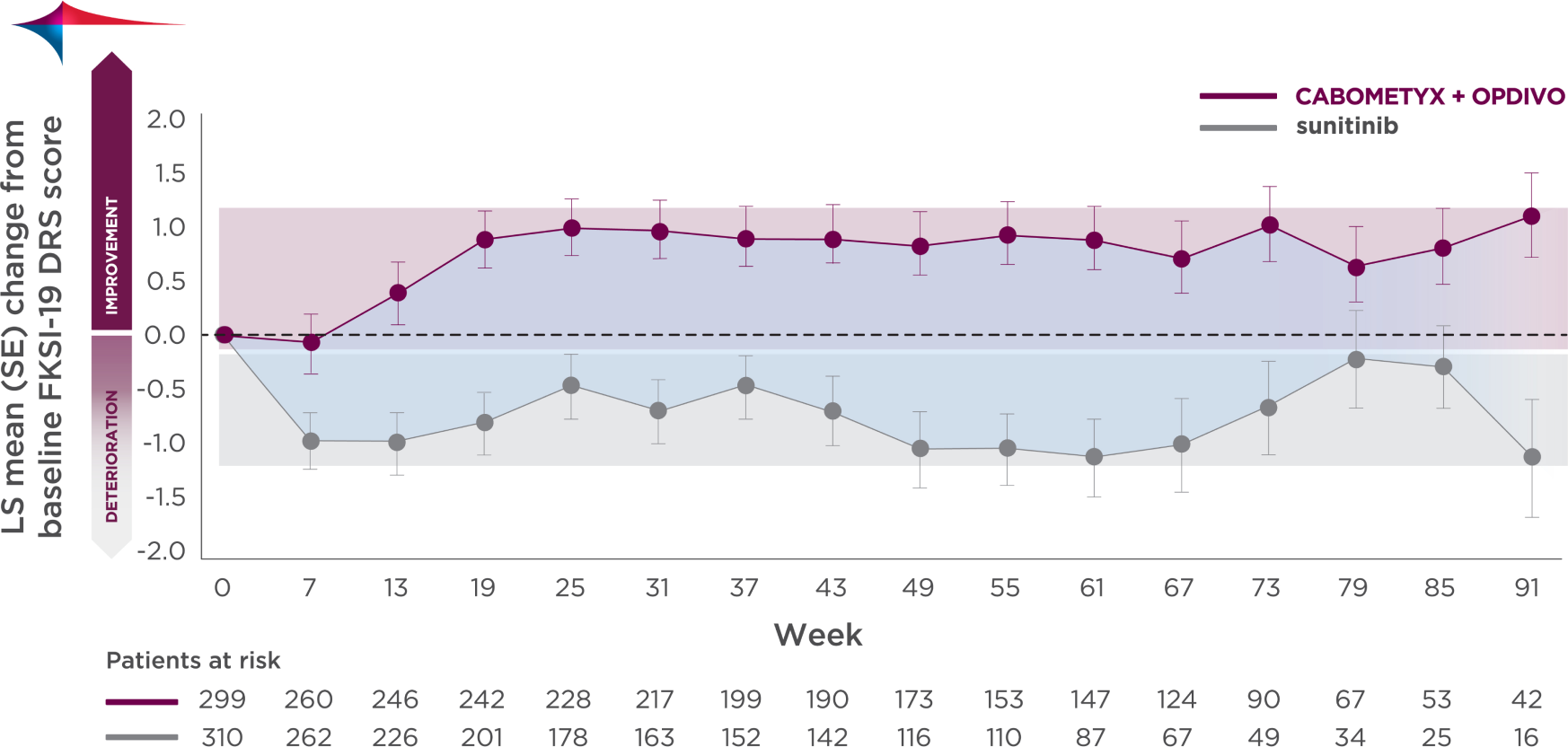
The clinical significance is unknown.2
Patients responded to statements about disease-related symptoms5
- I have a lack of energy
- I have pain
- I am losing weight
- I have bone pain
- I feel fatigued
- I have been short of breath
- I have been coughing
- I am bothered by fevers
(episodes of high body temperature) - I have blood in my urine
Mean changes from baseline for the FKSI-19 and subscales were prespecified. Least squares mean used above was done post hoc.2
The FKSI-19 total score scale and 3 subscales (disease-related symptoms, treatment side effects, and functional well-being) were collected to measure tumor-specific HRQoL. Change from baseline was assessed with the use of descriptive statistics, based on a linear-regression model for repeated measures that controlled for treatment group, time point, baseline patient-reported outcomes score, and the stratification factors (IMDC prognostic risk score, tumor PD-L1 expression, and geographic region). "Patients at risk" denotes ITT patients with baseline plus at least 1 post-baseline HRQoL assessment with nonmissing, patient-reported outcome data. Time 0 indicates baseline.1,2
FKSI-19=Functional Assessment of Cancer Therapy-Kidney Symptom Index 19; HRQoL=health-related quality of life; IMDC=International Metastatic RCC Database Consortium; LS=least squares; PD-L1=programmed cell death ligand 1; SE=standard error.
References:
- Choueiri TK, Powles T, Burotto M, et al; CheckMate 9ER Investigators. Nivolumab plus cabozantinib versus sunitinib for advanced renal-cell carcinoma [supplementary appendix]. N Engl J Med. 2021;384(9):829-841.
- Choueiri TK, Powles T, Burotto M, et al; CheckMate 9ER Investigators. Nivolumab plus cabozantinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2021;384(9):829-841.
- Rao D, Butt Z, Rosenbloom S, et al. A comparison of the Renal Cell Carcinoma Symptom Index (RCC-SI) and the Functional Assessment of Cancer Therapy–Kidney Symptom Index (FKSI). J Pain Symptom Manage. 2009;38(2):291-298.
- FACIT Group. NCCN-FACT FKSI-19 (Version 2). March 3, 2010. Accessed June 2, 2021. https://www.facit.org/measure-english-downloads/nfksi-19-english-downloads.
- FACIT Group. FKSI-DRS (Version 4). November 16, 2007. Accessed June 23, 2021. https://www.facit.org/measure-english-downloads/fksi-drs-english-downloads.